
“We are making a bet on obesity,” Lars Fruergaard Jørgensen, the CEO of Novo Nordisk, told investors in 2017. “We believe we can ride it based on lifting efficacy,” and that’s what will “create the market.”
Obese patients are “not hard to identify and diagnose, and they are all waiting for something that works,” Jørgensen told Reuters the same year. “I think we have some trustworthy bets.”
Bets. Betting. Creating a market. It’s the kind of language that plays well with financial markets and makes sense coming from a CEO (and trained health economist) who’s responsible to shareholders. It’s also the language of a man under pressure.
Novo Nordisk has a lot riding on its obesity gamble. No one has yet come up with a magic-bullet obesity drug, one that takes off significant amounts of weight and does so without serious side-effects. This includes the company’s own drug Saxenda.
Jørgensen runs the fifth-largest company in the global pharmaceutical industry, a company that last year generated $24 billion in global sales and a net profit of $10.1 billion (around the same level of profit as BHP). Built around the discovery of insulin, Nordisk was the creation of Danish Nobel laureate researcher August Krogh in 1923, which merged with its insulin competitor Novo in 1989.

Making medications that treat diabetes — one of the fastest growing chronic diseases in the modern world — meant the company improved the lives of millions of people. In the process, it created a licence to print money that made it much loved by investors, reporting double-digit sales growth year after year.
But Novo Nordisk’s fortunes took a dramatic turn in 2016, when a perfect storm of soaring insulin prices, increased competition, accusations of price rigging, and intense political scrutiny (see tweets by Donald Trump and Bernie Sanders) hit the US, its biggest market, derailing more than a decade of uninterrupted growth. Investors sent the stock price plummeting 40%.
The problems piled on in 2017. The company was forced to pay US$60 million (A$86 million) to settle a series of whistleblower claims stretching back to 2010. The company was accused of deceptive sales practices, of paying kickbacks to doctors who are high prescribers, and of downplaying the cancer risks of its main anti-diabetes drug. Internal whistleblowers alleged that sales staff were disguised as “diabetes educators” and that they received training from the marketing department before being sent to doctors’ offices.

With the company facing mounting challenges, including lawsuits alleging that it and two other companies fixed the price of insulin, it needed a step change: a new market that would promise investors the kind of mouth-watering growth that diabetes, now a crowded marketplace, had once delivered.
Enter obesity, a close relative of type II diabetes. An obesity product created the possibility of a crossover of drugs, but Novo Nordisk faced the same problem as everyone else in the market: it has proven devilishly difficult to make an obesity drug that is effective, safe and works at scale, across a population.
In a detailed investor presentation unearthed by Inq, Jørgensen set out the company’s strategy to dominate the market and lift sales — a move which Reuters reports would deliver roughly US$1 billion in profits by 2023.
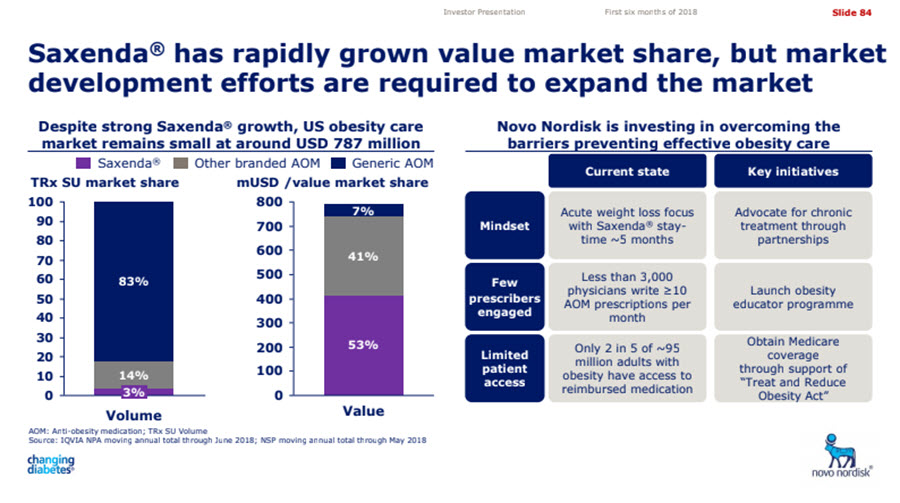
According to the 2018 roadshow presentation the company’s flagship anti-obesity drug, Saxenda, had rapidly grown its market share. But the presentation warned that “market development efforts” would be required.
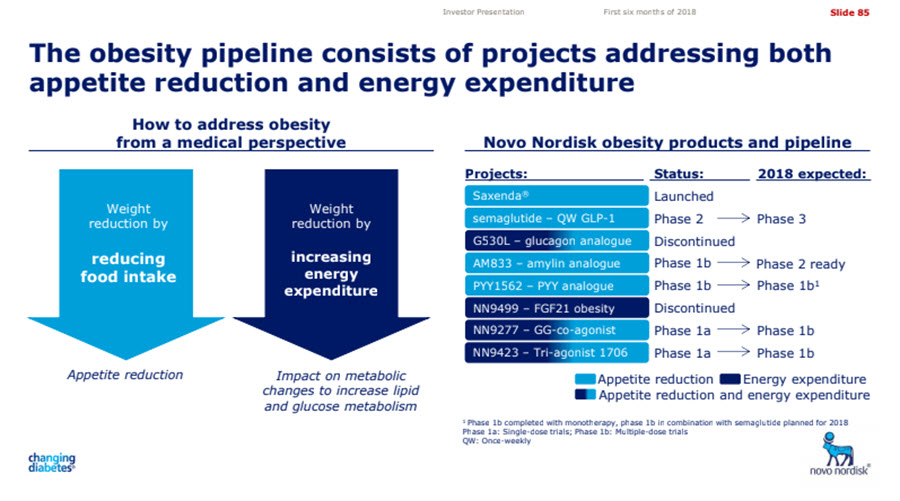
The presentation also revealed that the company’s scientists were at work on four new versions of an anti-obesity drug, in addition to the established Saxenda.
Its best prospect was a new drug, Semaglutide, which led to a claimed 16.2% weight loss during trials with apparently few side-effects. The drug has advanced to a third phase of testing with critical data expected in September 2020.
In an interview with US pharmaceutical website, Evaluate.com, Novo Nordisk’s chief science officer, Mads Krogsgaard Thomsen, admitted that the weight loss from Saxenda was “not phenomenal”.
“Today’s medications can only do around 10%, including our own Saxenda,” he said. According to Evaluate.com, the company was aiming for a result closer to that seen with bariatric surgery. “This can produce 30-40% weight loss, but is drastic and restricted to the most obese patients,” the site reported.
Novo Nordisk has told Inq that Australian law prohibits it from commenting on unregistered medicines.
In a statement the company said it had a “significant investment” in clinical trials in Australia. This included “a five-year cardiovascular outcomes trial, using a new investigational medicine, in people with obesity across 12 trial centres around Australia”.
It added that these new obesity medicines were “several years away from possibly being introduced to Australia and other countries”.
Tomorrow: How to win the hearts and pockets of doctors and pharmacists










If I had shares in this company I would ditch them already. Type II diabetes is now “treatable” with diet and exercise as soon as it is detected or diagnosed, and guess what, the same treatments apply to obesity, and metabolic syndrome. All these treatments are “free”. These treatments are all evidence-based, published in peer reviewed journals, and large scale trials are underway.
It’s time these pharma companies stopped trying to get people hooked on their products for the rest of their lives.
Sorry, I work intensively with people who have diabetes and diabetes is very often far more complicated than just diet and exercise. Pathologically it is a very complex disorder and over time can get worse regardless of how hard people work. Not that this means lifestyle factors are not important as they can delay progression but this does not always cure it.
I don’t know what work you do, but I am a type II diabetic and have managed very well without medication. Over time it need not get worse, if you stop eating too many carbohydrates. It is as simple as that. I am sure it is complex, but I am talking about type II specifically. Your standard ideas about it are based on no evidence at all, except the usual “take this medication” and we will manage it. Read some of the latest research in the area. Pubmed will serve you well. I have read that stuff. Sorry to point out that you are misguided.
Actually Totaram I am a Diabetes Educator and work full time with people with Type 1 and 2 diabetes. I definitely know what I’m talking about. For a great many people it does get worse particularly at the 10 year mark. I suggest you do some research. I’m not saying lifestyle measures are not important however when your ability to produce insulin fails as it does for many people with type 2 diabetes you are left with needing medications. Congratulations to you that this isn’t your journey.
“I know what I am talking about” doesn’t cut it. How do you know? What is the evidence? Why does the ability to produce insulin fall at the 10 year mark? Really? Not sooner? Does it depend on how well you control the blood sugar? Are you telling me that with a Hba1c of 5.4 in ten years I will need medication?
Why do you ask me to do research? I told you I have read the publications in Pubmed, but have you? Did you even read what I wrote? Why do you arrogantly assume you know so much? How do you know what my qualifications are?
Start from here:
https://www.ncbi.nlm.nih.gov/pubmed/30350061
[Remission is possible. Every patient with type 2 diabetes should have the right to reverse his diabetes!]
It’s in German, but you get the idea.
Is there a point to dragging this peripheral story into three sessions so far and more tomorrow ?
Plenty of other health issues to cover and plenty more angles on obesity for that matter. Not a great INQ start.