
A glaring loophole in the nurse-patient staffing model in states across Australia has allowed a number of hospitals to employ cheaper, underqualified nurses and pocket the proceeds, with some nurses warned to keep the issues under the radar and off the official incident management record.
New South Wales, Australian Capital Territory and Western Australia use a Nursing Hours per Patient Day (NHPPD) staffing model instead of a direct nurse-to-patient ratio, as used in Victoria and Queensland. (South Australia, Tasmania and the Northern Territory also use variations of the NHPPD staffing model, but haven’t reported similar issues.)
The NHPPD allocates each patient a number of hours of a nurse’s time — usually between six and eight — per 24 hours of a patient’s stay. But it doesn’t define a nurse’s skillset, meaning wards are left understaffed and underskilled when hospitals go cheap.
Qualifications not included
The legislation doesn’t specify nurse qualifications, says Christine Duffield, a former clinical nurse and professor at the University of Technology Sydney. “It doesn’t mandate the staff must be registered nurses,” she told INQ.
But even if registered and enrolled nurses are officially rostered, when they take leave — be it sick, annual or even maternity — there has been a growing trend to use an assistant nurse in their place. One investigation found nearly 7000 nursing care hours were missing across seven months in 2017 at the John Hunter Hospital in NSW.
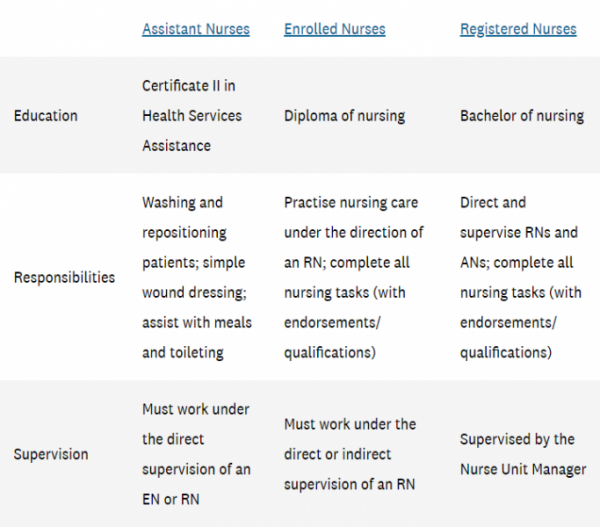
Assistant nurses can be as young as 16. They need a Certificate III in Health Services Assistance — a qualification which can be finished online in under six months. They can only complete basic tasks in care and must be supervised. Unsurprisingly, assistant nurses are significantly cheaper than registered or enrolled nurses.
It’s sparked rallies at hospitals across WA and NSW, with nurses demanding a like-for-like replacement model, while the ACT union branch has lobbied politicians for a mandated minimum nurse/midwife-to-patient-ratios framework.
Duffield says hospitals should never have less than 80% registered nurses on any ward at any time. “Anything below 80% registered nurses and you’d be getting into dangerous levels,” she said, pointing to a number of studies that show more registered nurses means better patient outcomes.
Hospital reporting worse for wear
When nurses want to report issues in NSW, they can either raise it with their manager or log it in the Incident Information Management System (IIMS). Biannual reports are then sent to the Ministry of Health for review, before being made publicly available on the Clinical Excellence Commission website (though no reports have been uploaded since 2017).
But staff at Concord Hospital in Sydney say they’ve been issued a directive from executives ordering them not to log staffing and unsafe working environment issues in the system. “The executive issued a directive saying not to log them in IIMS because it’ll be archived and told it would not go further,” one nurse unit manager told INQ.
NSW Nursing and Midwifery Association assistant general secretary Judith Kiejda says the issue isn’t localised. “The IIMS system can be rorted … Our members can put in that there was unsafe staffing, by either numbers or skills, but management can change that. There’s no way our members can print their reports off.”
NSW Health denied there had been directives for staff not to use IIMS for “perceived understaffing issues”. They added staffing was the responsibility of the local health district. “When an unplanned absence occurs it is not always possible to replace that shift with a nurse of the same category,” a spokesperson said. NSW Health declined to provide the number and qualifications of nurses hired per local health district.
Exhausted staff and patient risks
Nurses working on the ground paint a bleak picture. One nurse, who asked to remain anonymous, says she felt no progress was being made. “There’s a feeling of futility. What’s the point of logging [understaffing] if there’s not going to be action?” she asked. “I’ve made silly mistakes purely based on exhaustion and tiredness and I’ve seen other nurses do the same.”
Meeting minutes obtained by INQ show nurses who had taken five sick days between the start of the year and June were brought in for a discussion with management at Concord Hospital, while those who had taken eight days received a letter. Full-time nurses are entitled to 80 hours per year, meaning even those who had received a letter were well within their limits.
“I’ve found myself taking sick leave because I’m so exhausted I don’t feel like I could look after patients safely … But if I complain, I feel like it could affect my career. I stress about calling in sick, I stress about losing my job. My biggest stress is about harming a patient.”
Do you have information about this story that you’d like to share? Get in touch confidentially here.







The NSW Nurses and Midwives’Association have been campaigning about this for years. Privatisation of hospitals also stretches the resources of the union because agreements have to be struck with individual providers. About twelve months ago, the NSWNMA ran a very strong campaign to have registered nurses on all shifts in aged care facilities and it was voted down by the LNP in state parliament. The road to this state of affairs has been long. The outcomes of having overworked, understaffed, inadequately trained and supervised nurses will be very damaging and serious.
This is not only happening in the public system.
The private system is also bad, if not worse.
The public/ private model has been set up to circumvent the staffing ratios.
On a private maternity unit there is frequently rostered 2 midwives for a ward of 25 patients, and a delivery suite, the rest of the staffing contingent are a mixture of RN, EN and AN all of whom can perform some duties around the ward, but only the Midwives can look after perineum or cesarean wounds and breast feeding instructions and techniques.
I know of one patient who spent from Friday until Monday morning trying to get assistance with breast feeding her first baby to no avail. Her pediatrician arrived Monday morning, rolled her baby to the nurses station and said “This baby is starving, get him a bottle and help his mother to learn to breast feed.”
The private hospital is being paid at least $8,500 some funds pay $10,000 for the delivery and a private room for 4 days.
The private health provider is involved with other private/ public partnership hospitals and now is in the process of introducing a midwife lead model, which in Europe and the UK has significantly higher mortality rates.
One of the more entrepreneurial public/ private partnerships using a midwife led model, move the one day postpartum mothers and their babies into a motel across the road , with a ratio of 9 out patients to one midwife. The privately insured patient’s health funds are still paying the $8,500 to $10,000 and $2000 for the delivery to the hospital.
The midwives get upset, if the very busy publicly paid doctors won’t rush across a road to a motel room to manage a major bleed.
The doctors consider it dangerous to manage a complication in a motel room rather than an equipped hospital.
If there are any comments please google the skeptical ob/gyn.com to get more relevant data on the main driver of this Midwife lead model in Australia.
Agree ratty. My point about the NSWNMA’s resources being stretched to deal with this because of the large number of agreements that have to be struck with the private sector goes to the very bad problems you identify.
Vasco, most of the nurse and midwives in the private system in Queensland are not in the union, and this particular private health operator, luuurves Government money, with no oversight, because Queensland has no upper house and these partnerships are “commercial in confidence”.
They are also bullies and will happily destroy the career and reputation of anyone who stands up to them or dares to bring the head office into a problem, as the head office needs deniability.
Currently they are modeling themselves on the Vanderbilt hospital system, which is basically bullying incorporated with the arbiter of any complaint being the CEO or the Director of Clinical Services, who is nurse.
This provider does not think that it is cost effective to have a Director of Medical Services(doctor).
I know of one instance whereby the nurse who is the Director of Clinical Services, cancelled, clinically indicated necessary surgery on a patient, because a Midwife was anxious.
And so, whilst on holiday at 7.30 pm, only speaking to the midwife, the DCS (not a midwife) refused to accept a meta data analysis which supported the two specialists opinion and so, the surgery was cancelled.
The patient wanted and needed the surgery, because she had been in excruciating pain.
And so, I again say, the public/ private model is dangerous and it will take a long time for the real figures to emerge.
And then , comes the apology, the almost plausible explanation and its back to business.
If it was not people’s lives in the middle here, I could become cynical.
Yes but when it suits the Nurses Union in both QLD and NSW run the the line that the Assistants In ursing are superior to certificate 3 trained personal care workers. Many of the employers do the same thing and in some cases pay the personal care workers less than they pay the Assistants In Nursing (AINs)
Its another rort that is widespread in the Aged Care system as well.
At the same time in Aged Care many providers impose a mandatory registered nurse qualification on facility managers so the “Service Manager” counts as a nurse and due to the salaried pay arrangements can be said to be available and on duty. Check how many times the service manager actually attended on the floor or even paid a late night visit to a facilty to talk to residents or staff.
If this is not before the Royal Commission for Ageing, then it should be.
I have been horrified by what I have heard from the Royal Commission and yet, we still wait for any explanation, other than the professional apology, “We are sorry and we a working through the issues”, which means that they are sorry they got caught and will try to make sure they won’t get caught again.
Another question keeps floating through, If BUPA, a private series of companies, that has just recently agreed to pay some tax in Australia, can make a profit (and they do); why is the government not running these nursing homes themselves and save some money?
We have a family member in a middle management health care role in a quality, capital city public hospital.
Extension of shifts, which adds 2-5 hrs overtime, is common. Actually claiming overtime is discouraged in numerous ways. Surveys have shown that around 25% of young doctors fear that initiating an overtime claim could be career threatening.
This results in no systemic identification of OT, with no related assessment of extra resources required. Thus, additional staffing costs are avoided since there is no data to identify a staffing level problem.
So we have a health system and culture that creates fatigued nurses and doctors, accompanied by a management process that results in no data to justify extra staff.
Someone must be proud of themselves for keeping within their budgets. And suicide rates for young doctors continue to climb alarmingly.
Older doctors are often aware of the current situation, but a manager of a medical centre commented to me – The older doctors thought they came up through a tough old school of mentally fatiguing hours and systemic blind eyes to overtime, so the young doctors can do the same too.
Just great, Huh?
To a degree what you say about the more senior doctors is true.
The theory behind the “work them until they drop” is that junior doctors, in training, have senior doctors on call to bail them out if the situation becomes complex or they can’t cope with the situation.
To my memory as junior training specialist registrar, my husband would volunteer to be the medical assistant in operations he had not seen done before, working many hours for the experience, rather than the money.
As a senior registrar he would frequently work as the lead surgeon, with a junior registrar as his assistant.This surgical time was part of enormous hours, such as a 36 hour shift.
The hours were brutal and the stress almost mind boggling, and yes, it was a case of anything that doesn’t kill you makes you stronger. It also refined the ability to think critically, make decisions decisively and perform when drop dead tired.
I am not sure that the suicide rate has risen over past years, for junior doctors, because for a long time we didn’t speak publicly about the suicides. There has been a significantly large number surrounding one of the private health providers, and these people were senior staff. I probably am mistaken about the student numbers.
I don’t know what we have done with our child rearing or our education system, because we are graduating medical students that lack resilience and also lack basic life skills, such as introducing themselves to patients, rephrasing their advice if the language used by them is too sophisticated.
The idea that they are somehow special because they have gotten into the medical course and passed it, certainly needs to be washed out of them before they have patient contact.
Returning to the brutal hours, which are supposed to be “safe” working hours, these have essentially resulted in lots of specialists who have graduated with less than one third of the operating and face to face hours of previous generations of specialists.
My husband has been one of a group that have had to mentor newly graduated specialists, who in essence are not safe to work on their own. It has happened on more than one occasion where a Specialist is sobbing in theatre “Get so and so to help me, now”.
There has been arrangements made for someone to come straight out of their training and into working solo in a small private hospital, which doesn’t actually have a crash team. This arrangement was made between the CEO and a junior registrar.
Private health providers want very young and inexperienced doctors on staff, especially if they are going into a public private partnership hospital, because they are ripe for exploitation and will do as they are told, whilst remaining gagged to disasters they have seen.