
Amid all the healthcare news of late, the most significant shift in Australia’s medical sector has barely been debated or widely understood. The Australian Competition and Consumer Commission’s draft decision giving health fund Nib more leverage — and the purchase by Medibank of stake in both a private hospital and a chain of practices — will mean that health funds will get more say in how care is delivered. This signals a seismic policy shift in the private healthcare sector.
The provider lobby, led by the Australian Medical Association (AMA), is reacting strongly, claiming that such “managed care” will reduce care quality and compromise outcomes.
The claims are made as self-evident and tend to escape proper scrutiny. This isn’t right given what’s at stake. Let’s not forget that the Royal Commission into Aged Care Quality and Safety cast serious doubt over the wisdom of leaving providers of an asymmetric service to their own devices and with little oversight.
But healthcare is different, right? Medical decisions are always based on the best evidence and reflect only the needs of the patient. Actually, there’s much Australian data suggesting otherwise, especially in the private sector.
The medical postcode lottery
In the absence of reliable data on outcomes (an ongoing hindrance to good practice and policy), one way to flag potential problems is by measuring standardised differences in service provision between regions. While some variation is warranted, dramatic disparities can indicate problems with medical practice and/or lack of access and facilities.
Analysis by the Australian Commission on Safety and Quality in Health Care suggests that we might have a problem. For example, an adult living in Dubbo is 56 times more likely to undergo a heart perfusion scan than someone residing in Onkaparinga, South Australia. This is after adjusting the data for demographic differences. Neither region is classified as remote, so lack of service availability is unlikely to be a major factor.
Is it down to levels of heart disease? Perhaps, but it’s very unlikely to explain such magnitude. In fact, a 2016 variation study (using the larger geographic units of Medicare Locals) found surprisingly little geographic association between the rates of coronary angiography — another cardiac investigation — and levels of heart disease. However, a strong association between angiography and private hospital admission was found. This suggests factors other than medical ones play a part.
In addition to unwarranted variation, too many “low value” procedures and tests with little proven clinical benefit are commonly performed in the private sector. Some of these have now thankfully been amended or removed from the MBS as part of the recent review.
And then there’s questionable adherence to clinical standards and guidelines. Two peer-reviewed Australian studies looking at common adult and child health conditions found that clinical encounters complied with best-practice in fewer than 60% of cases on average.
While such problems are not unique to Australia, the causes can be distilled to the changing nature of healthcare and a private sector funding model that encourages volume over value.
It’s not a cottage industry any more
Healthcare has changed. Good care is no longer the sum of individual medical interactions. Not only are patients now medically more complex — with multiple health problems that require sustained management across disciplines and professions — but biomedical science and knowledge is vast and expanding rapidly.
Safe, high-quality care is now therefore a team sport and the collaborative model works best when GPs, specialists, nurse practitioners and the patient use the same electronic platform to communicate and view results and medication updates.
This approach is highly suited to “provider networks”, which can offer the necessary central administration and management. It also happens to be a key feature of managed care and a departure from the quaint sole practitioner model of yesteryear.
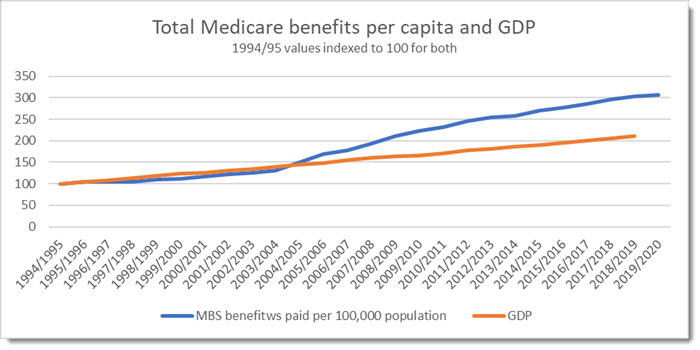
Every dollar of expenditure is a dollar of income
The Australian private health sector is characterised by a fee-for-service payment model (based on interventions, not diagnoses) along with a firm separation between payers and providers.
This combination encourages growth in activity and in fees, with little incentive for restraint or value. There are currently no limits on what providers can charge, and ample evidence suggests that they will lean towards options that generate the most revenue rather than alternatives that are more conservative but equally effective. There’s also little association between medical fees and quality. Higher costs, meanwhile, are borne by insurers, patients and — via Medicare — the taxpayer, reflected in growing premiums, out-of-pocket costs and Medicare expenditure.
Now, there is no question that health professionals believe that they act in their patient’s best interest. But they are human, and healthcare is very complex. Research shows that they are often unaware that treatment may be inappropriate or even harmful, and that medical decisions are driven by a range of incentives, including financial ones.
While concern about insurers owning hospitals is understandable, the opposite is also true: provision that is completely decoupled from financial risk can generate overtreatment and higher costs with little value added.
This is tempered if the payer has some say in what and how care is provided. For example, joint replacement using a short-stay model produces the same outcomes as a longer, more expensive admission. Patients prefer it and it’s cheaper overall, but many private sector providers resist it — despite it being routine in the public sector.
Nothing radical or dangerous about it
Israel’s health system is considered among the best in the world. It’s also comprised entirely of health maintenance organisations (HMO) — payer-provider entities that are a feature of managed care.
Clalit Health Services, Israel’s biggest HMO, looks after 4.6 million people who receive excellent care when needed, but also cutting-edge preventative interventions designed to keep people healthy and out of hospital. It is in both Clalit’s and the patient’s interests to do so. The excellent analytics are due to an enviable, all-encompassing dataset on enrolees’ health, care and lifestyle factors (which, incidentally, enabled the lightning-fast observational study of the Pfizer vaccine). This is unimaginable in the Australian system.
Under the much-maligned US system, the payer-provider model has actually been a success. Kaiser-Permanente delivers evidence-based, efficient care and excellent outcomes without breaking the bank (or bankrupting the patient). Health professionals employed there are actively involved in generating patient care pathways and enjoy being part of a system that is focused on outcomes. The result? Coordinated services involving screening, prevention, primary care, outpatient care and hospital care — again, impossible under the fragmented Australian system.
In fact, we already have good examples of payer-providers in Australia. Public hospitals are both funded and managed by state and territory governments and perform very well. Plus, let’s not forget that the aged care royal commission found that public facilities provided better quality care than their private counterparts.
Striving for better healthcare for all Australians
Giving payers more say in how care is delivered is not a silver bullet. If we really wanted to improve patient choice and care quality we could enforce much more transparency on medical fees, mandate routine data on actual outcomes, and explore remuneration models that reward value over volume.
But it isn’t a radical change, either. It’s how public hospitals are managed and Medicare already dictates what can and can’t be done privately.
Dismissing it without debating the evidence has a whiff of “nothing to see here” and is a wasted opportunity to at least explore how to improve Australian healthcare.
What do you think? Do we need to examine alternative paths to our healthcare here in Australia? Write to letters@crikey.com.au, and don’t forget to include your full name if you’d like your letter to be considered for publication.
Luke Slawomirski is a health economist, most recently with the Organisation for Economic Co-operation and Development (OECD) in Paris. He lectures in health policy at Imperial College London, is a former clinician, and a visiting fellow at the University of Technology Sydney. He worked at the Australian Commission on Safety and Quality in Health Care between 2011 and 2015 and was a co-author of the 2016 study examining coronary angiography in Australia.
This article benefited from input by orthopaedic surgeon Ian Harris, professor of orthopaedic surgery at UNSW and honorary professor at the University of Sydney‘s School of Public Health.







“Patient choice” is a very common term in these sorts of discussions, and a key phrase whenever the subject of private hospitals and health insurance comes up. I don’t understand it at all. I don’t want choice. I just want competent medical care on whatever rare occasions it’s needed. I certainly don’t have the medical training necessary to understand or rate any choices that might be available, and I doubt that many in the community do.
In this particular instance the woman (patient) wanted and needed the surgery, the hospital had the staff, the theatre and the surgeon.
Another nurse spent almost 4 hour wailing that it was too dangerous and contacted the nurse with the title of Director of Clinical Services who was on holiday and supervising the hospital from wherever.
This person made the “call” at 8pm on a public holiday and refused to speak to either the surgeon or the specialist looking after this woman.
The public hospital system was worse, as the patient was transferred to a surgical ward and didn’t see a doctor for 3 days as she became yellow in skin tone and suffered excruciating pain.
I tend to agree Andrew. I had a career as an analyst (anything and everything) and people are very poor at even making informed choices. On medical procedures, information asymmetry is the standard, and asking for a second opinion is always a choice but is also usually a bit expensive and a pain to arrange, especially for specialists.
I do however remain confident in the public system for anything that is a genuine emergency, although noting ratty’s example which can happen from time to time. I wonder if ratty’s friend was in the public system or one of these wonder private hospitals.
What a fantastic and refreshing read!
it’s a pity I’m not entirely convinced of the benefits of the managed care in our weirdly hybrid system however. I also live in perpetual fear that the private system (whose maneuverings have prompted this debate) is simply adopting the managed care model to shore up their profit. Their current behaviour is not really focussed on patient outcome so much as it is cost. This reduces choice, encourages siloing and centrality of data behind a pay-wall, and can incentivise providers to maintain lower quality procedures with more side effects rather than adopt newer procedures that bear a premium.
I am very suspicious of the health world. I suspect there are a lot of things going on to rort the system to get medicare money. 2 years ago had a skiing accident. Got a referral to a doctor in Melbourne from the practice on the mountain that charged like a bull. By the time I finished I had had an xray, an ultrasound, and MRI, a cat scan and a consultation with a specialist each time. All up about a dozen professionals took a bite out of the Medibank pie. Then end result, too little damage to intervene. No action taken. Still sore two years later although it is improving.
I am also concerned about big pharma rewarding doctors for prescribing favoured high margin products regardless of efficacy. Can big pharma access data of what doctors are prescibing? Are doctors receiving secret commissions?
As a former car fnance salesman the providers of the finance products used to reward me big time for selling their products. This has calmed down since the banking royal commission exposed this as a rort.
Is something similiar going on in pharmaceuticals? My guts tells me it must be but how to prove?
DIrect kickbacks to doctors for prescribing particular medications are illegal but doctors can be invited to some very enjoyable conferences and given certain gifts with “no strings attached.” This kind of relationship may, even unconsciously, affect the doctor’s choice when prescribing.
Let us start with the metric of “Managed Care”.
Who decides what is actually the best way to decide the type of care and the examinations required?
The whole of both the private health system and the public system is littered with nurses who have done some further management training, masquerading as a medical Doctor.
Yes they have their PhD in some esoteric aspect of nursing or management and then they are employed into management roles with titles such as “Director of Clinical Services”.
I know of an instance where one of these nurses with the title of Director of Clinical Services took it upon herself to cancel emergency surgery that two specialists deemed very necessary, with blood tests indicating a possibly ruptured gall bladder.
The patient eventually had the surgery done after 4 weeks of excruciating pain and massive amounts of antibiotics.
She was and is still suffering from an infection which has grown up into her liver.
This disease process has a 18% mortality rate in Australia.
Tell me again, how this was the best outcome for the patient.
“A private sector funding model that encourages volume over value”