
Heart problems are one of the biggest killers in Australia — and not just for old people. They are one of the leading causes of death for those who would otherwise have plenty of life left. If you’re a man aged 45-54, the most likely thing to kill you is what they call “ischaemic heart disease”.
COVID is well known to affect the heart during acute infection — and leave it weakened.
“[A] significant proportion of those with prior COVID-19 infection also exhibit signs of cardiac damage,” write Corinna Serviente, Stephen Decker and Gwenael Layec in their 2022 paper, “From heart to muscle: pathophysiological mechanisms underlying long-term physical sequelae from SARS-CoV-2 infection“.
Was the death of Shane Warne earlier this year a forewarning of a wave of post-COVID heart attacks in men who’d rather grow old enough to meet their grandchildren? With the release of official Australian Bureau of Statistics data on causes of death in 2021, we finally have information on what is happening in Australia.
It looks concerning. The standardised death rate from heart diseases rose in 2021 compared with 2020. It rose for men who are particularly prone to severe COVID infections due to the higher prevalence of ACE-2 receptors in their body. But the standardised death rate for women rose even more.
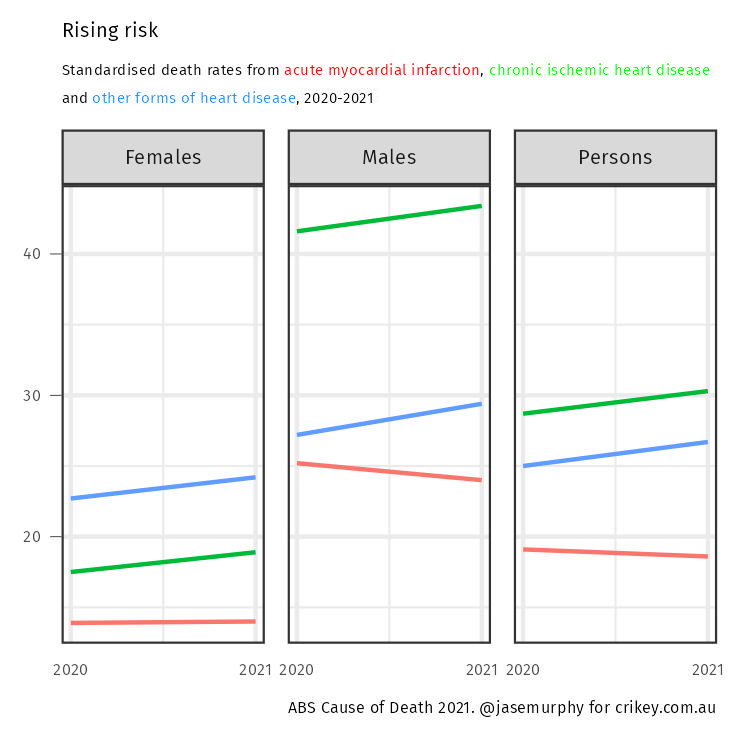
What the chart above shows is that heart problems soared, but the chance of clutching your chest and falling to the floor did not. While heart disease is up, acute heart attacks are down. (Myocardial infarction is just a fancy phrase for a heart attack.)
It is important to understand what the graph above shows: a standardised death rate.
Calculating a death rate is a way of accounting for the fact we have a larger population each year. You’d expect the raw number of deaths by heart attack to rise each year; using a rate controls for that. Standardising that rate is a way of accounting for the ageing population.
We have more old people each year. You’d expect the raw number of deaths by heart attack to rise as the population gets older, but if the risk in each age group isn’t changing, you want the standardised death rate to stay the same.
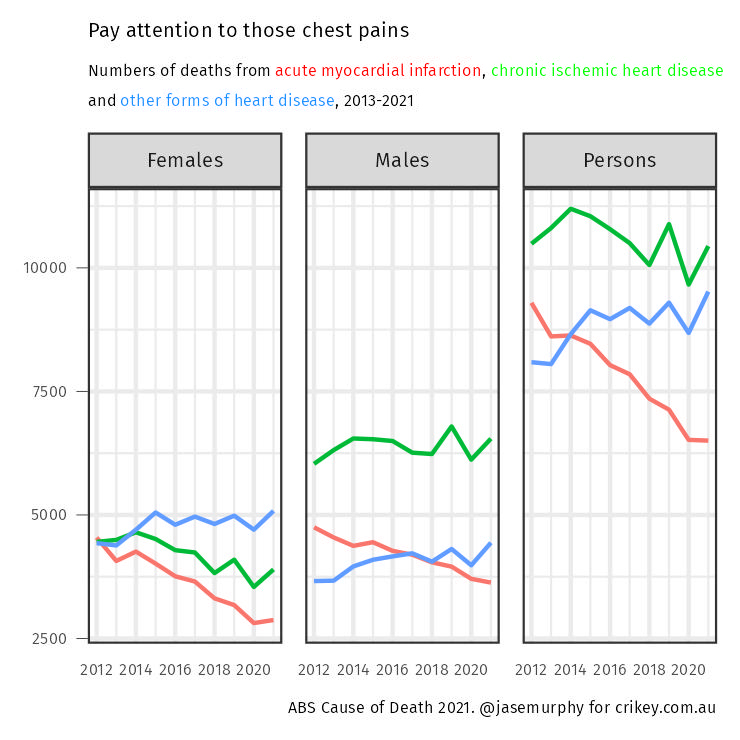
Of course, comparing 2021 with 2020 could be misleading; 2020 was a year with very few deaths. If we look at the bigger picture, we find something interesting. As the next chart shows, ischaemic heart disease deaths and heart attack deaths are falling over time. This makes the change in 2021 a little more concerning — it occurs against a backdrop of decline. Other forms of heart disease have been pretty stable recently before rising in 2021. Also concerning.
But this data is from 2021, and won’t contain all the December deaths from the COVID waves that hit Australia in 2021. The data shows deaths reported last year, not deaths that occurred last year.
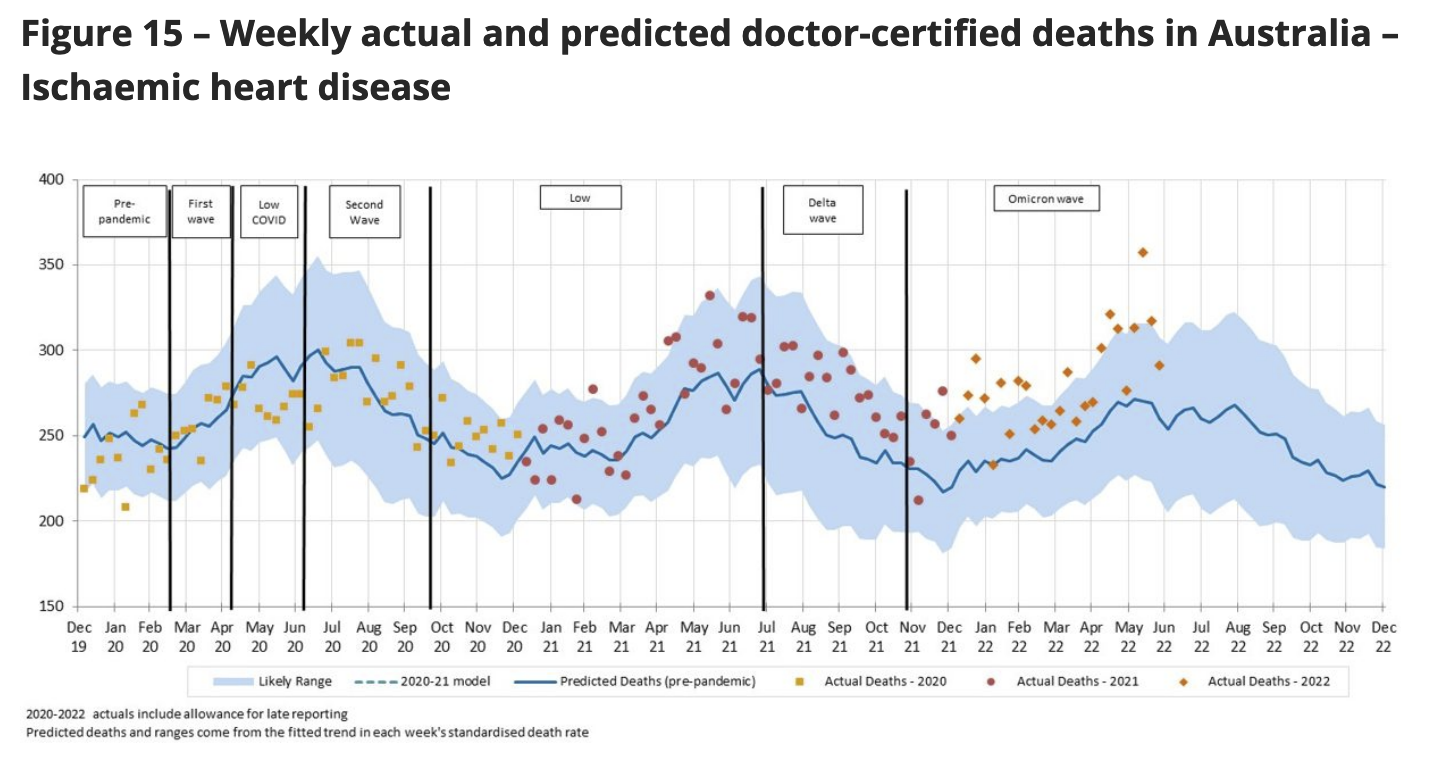
What do we see if we look at newer data? The Actuaries Institute has been diving into the latest data and analysing it against its expectations of how many people would usually die of heart problems. It finds a 12% increase in deaths from ischaemic heart disease so far in 2022.
As the next chart shows, deaths from heart disease are clearly above their estimated baseline.
This matches data from the US, where COVID was much more prevalent much earlier and where heart disease has also risen. Scientists find people who had COVID are more likely to have heart failure and (in contrast to Australian data so far) heart attacks.
Scientists warn of “a substantial increase in global cardiovascular disease burden as SARS-CoV-2 continues to spread throughout the population”.
It seems likely cardiovascular doctors of Australia will be very busy in 2022 and beyond.
So what can be done?
Scientists don’t have specific recommendations yet, but the risk factors for heart problems remain relevant. If you’ve had COVID and never done a spot of exercise in your life — or if you smoke — it could be time to finally make a lifestyle change.
Are you concerned about the after-effects of COVID? Let us know your thoughts by writing to letters@crikey.com.au. Please include your full name to be considered for publication. We reserve the right to edit for length and clarity.







I’d had a heart attack in 2010 – lost about 25% strength in the left upper bit, so lost some strength overall, but otherwise, I was OK. Developed Atrial Fibrilation end of Feb this year – had tests, heart function reasonable, booked into Cardiologist. Got Covid!
When I thought I was going to die after 3 weeks – couldn’t breath, knackered, went to hospital. Spent almost 3 weeks in hospital while they battled to get my heart stabilised, heart function down to 25%., but I was still alive. Also had Liver indications as though I were a heavy drinker (I’m not) and almost had renal failure, apparently! After they patched me up (liver and kidneys improved as CV was flushed out of system) and tossed me out of hospital, finally saw my new Cardiologist! He was appalled. After a drug regime to get my resting heart rate down (from 109 to 62), will try cardioversion (electrical shocks to heart to try and get it back into regular rythmn). If that doesn’t work, it’s a pacemaker! At least heart function is back up to 38-39% – from 49% earlier in the year. Other lingering effects of CV were feeling as though the top of my head was encased in cotton wool, for about 6 weeks, and find it harder to concentrate. Yes, I had 4 shots. Who knows if they were effective, or affective.
drastic – yes, my heart attack felt like a bit of indigestion – no real pain – started feeling crook so went to emergency at 2 in the morning – sent to Royal Perth H and they found a full clot up by my heart! – can still recall one surgeon saying “this guy should buy a lotto ticket”.
Very sorry to hear this, hope you have a better run now.
Please be warned – plenty of heart attacks are painless. Sudden onset of feeling ghastly is pretty reliable.
The blunt reason Australia is not yet demonstrating the effects of Covid19 infections is that we kept our population insulated until we had a vaccine which mitigated its effects.
Then our government reluctantly provided anti-virals to limited numbers of the most at risk population.
Give it time, and the same results will show because the “Let it RIP” group headed by Nick Coatsworth has let the genie out and it is not going back.
Yep, we were doing remarkably well (despite the LBP letting the virus in courtesy of Alex Hawke’s friends who wanted to disembark from the Ruby Princess), thanks to some rare cooperation between governments and actual attention paid to actual experts. Sadly that attention waned, but at least by then we’d had some vaccine protection in place.
Jason, you can’t write this story without referring to the other novel factor: the widespread use of experimental mRNA vaccines, especially booster shots, which occurred over the same period. The web, especially social media, is alive with anecdotes concerning unexplained excess death rates, vaccinated athletes dying from heart attacks, funeral directors reporting on changes to the demographic price of deaths referred to them and individuals who posted to social media decrying anti-Covid vaccination sentiment and reporting that they were about to do the right thing and have their booster – only to die within a week or two.
You may well dismiss a role for vaccines in these tragic deaths, but you can’t dismiss the issue without appearing evasive.
At the very least, there should be post mortems on all these deaths – and probably a public inquiry.
“Price” should be “profile”.
My daughter-in-law and son were surprised when I pointed out that mRNA vaccines had been in development and phase 3 clinical trials for about 10 years prior to this pandemic, with the express intention of being used in children for cancer therapies.
There was/ is nothing “new” about mRNA vaccines, except for the publicity given to them, when they were re-purposed for SARS CoVid19.
The key word here is ‘anecdotes’. As the saying goes, the plural of anecdote is not data.
Don’t get too locked in to that cliche’d response.
Thousands of anecdotes from all over the world that reflect personal experiences and tragedies that run counter to the establishment’s presentation of events should be a signal to a responsible establishment to take notice, acknowledge the concerns and investigate.
Yep, let’s not just mention the elephant in the room…
From The Lancet (June 2022)
’Similar to previous studies, Wong and colleagues observed higher than expected rates of myocarditis (and pericarditis, a closely related clinical presentation), specifically in individuals younger than 35 years, with the highest risk among men aged 18-25 years after their second COVID-19 mRNA vaccine dose.
Thanks for the reference. It was reassuring to read:
The clinical presentations of myocarditis after COVID-19 mRNA vaccination have been predominantly mild and few patients have required intensive treatment.
Hopefully such events are ‘predominantly mild and few patients have required intensive care’. I’ll await more research on that.
However, this finding should not mean that such events are entirely ignored in broader discussions, like this article, regarding adverse outcomes related to the ‘vaccine’.
Are you volunteering for a repeat of phase 3 clinical trials to see if you develop myocarditis / pericarditis?
The most common presentation for both these conditions, in Australia, are people presenting with Rheumatic Fever and who then go on to develop Rheumatic heart disease,
This is a complication of Streptococcus A throat which is highly contagious and susceptible to penicillin based drugs.
Over 20 years of research, development and testing of modern mRNA vaccines does not make them experimental. They first ones developed in the 1970s, for crying out loud. Just stop with the discredited anti vaxxer rhetoric.
While anecdotes don’t substitute for phase II clinical (Human) trials, they can point to products/therapies that would qualify/deserve to be tested. There are OTC products for sale that have demonstrated effectiveness in the test tube and anecdotally, and whose ingredients have shown positive phase II trial results. But without the $10million or so required to do a 300 person phase ii clinical trial of the actual formulation, they can only be sold as supplements, and cannot be advertised as :effective”..