
The aged care taskforce report, with its recommendation that seniors be required to pay a significantly larger proportion of the costs of aged care rather than all taxpayers carrying the responsibility, has debuted this week to relatively little angst.
That will change when the government reveals how it intends to implement the recommendations around a pension-based mechanism for co-payments for “daily living services” in aged care, in contrast to caring services, which the report recommends be fully funded by government, and if it adopts the recommendation to allow providers to keep a small portion of the Refundable Accommodation Deposit that clients can currently use for their accommodation costs.
Judging by the hysteria from wealthy seniors, and the media coverage of it, when Labor proposed to take away their franking credit rort in 2019 — who can forget ABC’s 7.30 program interviewing an angry retiree on his yacht? — there may yet be a political storm at the next election, especially given wealthy seniors are a key Liberal constituency. Peter Dutton might decide to campaign on ensuring taxpayers continue to fund the aged care costs of wealthy Boomers.
That would leave the Coalition with the problem of funding the mammoth and rapidly increasing costs of aged care afterward, but it could fall back on the traditional Coalition approach of letting the system run down until a kerosene baths-style crisis erupts at some point in the electoral cycle beyond. Or it could decide, in the spirit of Tony Abbott attacking Labor’s middle-class welfare cuts only to impose even bigger cuts himself, to make wealthy seniors pay anyway. What are they going to do, vote Labor?
Nonetheless, there’s been a significant policy shift that has made and will make aged care less challenging. Getting people to age at home as long as possible has long been seen as the key both to minimising costs and maximising community and individual benefit. A form of home care package was introduced by the Keating government in 1992 and various forms of home care funding have been expanded ever since. The whole home care package system was overhauled by Julia Gillard in 2012 following a major Productivity Commission report, making it more client-centric and expanding it further. In the wake of the aged care royal commission, the system is again being overhauled so that by 2027 there’ll be a single Support at Home program with greater flexibility and a single provider invoicing the government against a set budget for each client.
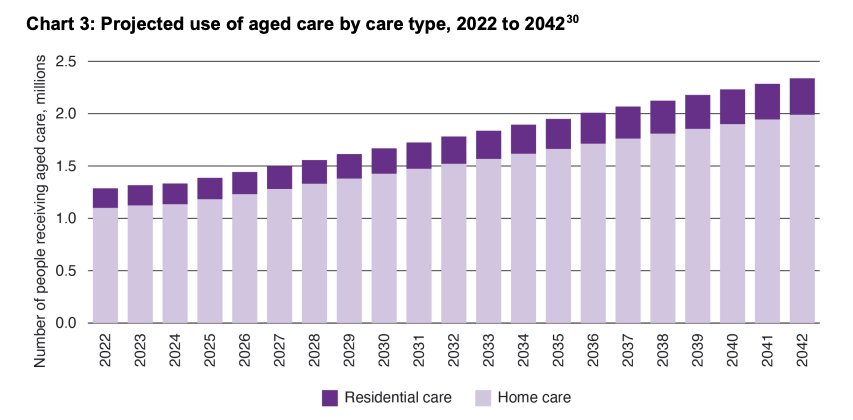
The aged care taskforce shows that home care is the future of aged care. In 2022, for the first time, there were more recipients of home care than in residential aged care. While we’ll always need the latter, it is only projected to grow by a relatively limited amount in terms of the number of users over the next 20 years, whereas the size of home care will nearly double.
This has big implications for the sector. Home care is more attractive to both the private sector and not-for-profits: according to the taskforce report, “69% of residential aged care providers made an operating loss in 2021–22, an increase from 54% in 2020–21”, whereas “in 2021–22, 69% of [home care] providers reported an operating profit”.
Home care also requires fewer workers given there is no need to provide accommodation and support services. Currently, residential care employs nearly 280,000 workers, while home care employs 156,000. Funding home care is also much less complex, without the sensitive issue of accommodation bonds and raiding super or the family home to provide a Refundable Accommodation Deposit.
Home care also offers a simpler split of services and funding requirements. The taskforce says governments should pay most, or all, of the clinical/caring components of home care, there should be a more even split of independence-related services, and clients should pay most of the costs of ordinary living services they’d pay even if they weren’t in a home care program — such as cleaning.
But as home care comes to dominate aged care, it comes with its own problems. It is competing with the NDIS for a workforce — the taskforce deliberately shied away from the long-running and vexed issue of the aged care workforce, saying it didn’t have time to do it. Vetting service quality is more difficult than with residential (especially large residential) facilities, which can be spot-checked by the quality regulator. The home care sector rapidly grew as governments increased funding through the 2010s, but it has now entered a period of consolidation, which may weed out some of the more exploitive operators. However, the combination of government funding and potentially vulnerable clients in their homes will continue to present a tempting target for the unscrupulous.
For policymakers and the public at large, we need to change our conception of aged care. Soon it will no longer be about nursing homes, it will be about home care, with residential care as an end-of-life adjunct. And that’s a quite different industry.







I have a 93 y-o neighbour who has been in an ageing-in-your-own-home program for several years. She has had home cleaning, gardening and shopping help although, after a recent sudden decline in her mobility, has stopped shopping with a support helper and the helper now does the shopping for her.
Her house is compact, has a wide enough corridor for wheeled walking support or a wheelchair should it become necessary, is all on one level and undercover parking is very close to the front door and she has lived in this neighbourhood for about 30 years.
She has family in the next suburb and across town and several long time neighbours drop in regularly and are on instant-dial contact.
It seems to be a good model and certainly works for her.
But the problem has been what BK refers to as “competing with the NDIS for a workforce”. Plus Covid was an issue that brought its own set of problems. Her supporters/helpers have changed many times, often with little notice, and sometimes expected helpers have not arrived. I suspect that much of the money goes to the middle “men” (and from the interview on 7:30 I gathered that these “interests” made up a large portion of the taskforce membership) rather than to the workers who seem to be largely “gig” employees.
So while it has been a much better solution than moving to aged care would have provided, the problems of finding, and retaining, suitable skilled staff dominates all care sectors – child, disability and aged care – alike.
You look to have nailed it. As has your neighbour.
Every time the government hands over responsibility for a social service to the market of privatisation it becomes a scam, sooner or later. It’s inevitable. Very expensive beans on toast.
Last time I was in hospital (last year) I asked why occupational therapists and social workers are in such short supply and was told that is because the NDIS pays them a lot more money. No wonder the NDIS budget is blowing out – it is the providers who are gaming the system.
You are extremely wrong, the vast majority of OTs and social workers work extremely hard for relatively little pay. The ones rorting the system as someone said above are the middle men, the private companies whose main aim is profit.
In my extensive experience with aged care, such professions leave the public health system and set up a private business, whereupon they then draw on the aged care package (and NDIA) honeypot, overcharging anywhere between 25 – 150 per cent more than what they would for someone not on an aged care package – the system has been rorted by these and other health professionals since this lucrative package system was introduced many years ago. This is but one of the many fundamental well known flaws within this system, there are many more that are equally bad and even worst, particularly such ‘flaws’ that disadvantage the elderly person further by limiting or denying access to their aged care package funds, impacting their health and wellbeing. I’ve seen and heard many a horror stories over the years, and still there is no let up, despite a Federal change of Government and Royal Commission – Package service providers and those private business health providers have a lot of clout in Canberra. I suggest that your readers get on- line and google some of the Aged Care Package service providers out their, and look at reviews and government audits pertaining to these services, it is truely a disgrace and a waste of public resources, resources if used properly and with greater transparency, accountability, and with vastly improved service provide penalties for wrong doing (that includes prosecution and jail) would indeed save many elderly lives and alleviate a lot of suffering for these elderly citizens and their involved families. There is sooo much ongoing blatant rot and rorting of this system that it’s hard to believe that this system has not yet been rebuilt or at least significantly restructured – to the great disadvantage of our elders, are those vested interests welding their power in Canberra for their own greedy benefit.
Tony, I’ve worked inside the various systems for fifteen odd years now and…you are right. Most people have no idea of how lucrative the care sectors now are, if you have no scruples and are very cunning in the way you play the Middle Class Guilt card.
The fiscal moral hazard and the systemic double standards – and the care disparity injustices they enable – would appal most Australians.
Herein lies the nativist wedge to preclude effective recruitment and staffing, when we do not have sufficient working age ‘demographic powder’.
The same ‘immigrants’ needed along with local workforce, and as used in EU nations, have been dog whistled via RW MSM & parties for a generation and by many of the same oldies or voters needing home based aged care?
In in the age group where all my friends are experiencing or have experienced their parents going through the aged-care package and/or aged care facility stage of life. Pretty much none of it is good. No matter how good aged-care facilities are, they’re still “god’s waiting rooms” where the clients have almost no agency, and understandably are often bitterly resisted. So the cleaner comes, the gardener comes, someone comes to make sure they don’t slip over in the shower, the kids and grandkids share around the never-ending trips to GP’s and specialists, and various scanning and testing facilities, but so often one of the olds falls over. Then it’s a stint in hospital, rehab, OC’s, etc, or maybe a hip replacement etc, and they cost the taxpayer even more than usual. And in the meantime, many, like my parents, are rattling around in a 1950’s four bedroom suburban home that should have been freed up for a younger family decades earlier. Yes, when the time comes, I’d rather be cared for at home myself, but it’s not a perfect system. One thing is for sure, we’ll all be paying more for old age.
Thanks Bernard, that’s really interesting. I don’t understand that graph though: you say “In 2022, for the first time, there were more recipients of home care than in residential aged care,” but the graph seems to show home care outnumbering residential care in 2022 by about five to one, and they both seem to roughly double from there.
YOU SHOULD KNOW THE PICTURE TELLS THE STORY! How dare you actually think about the problem. I noticed the possible error but was too lazy to go further.
Hmmm. Crikey could start by making their comments section easier for us old folks. We don’t like change. Having worked in the industry before I became part of it I was intrigued by the number of migrants being recruited. Predominately Filipino. Recently read an article in Crickey where it said migrants were a substantial contributor to a less equitable society.
Then there was the case of the extended family. Elderly gentleman used to drive to the Bowlo and have three beers in about three hours. Just for something to do. Daughter thought dad should not drive and had his drivers license cancelled. COVID hit and he decided to just stay in bed and stopped taking his medication. Was found and recovered but transferred to a nursing home and just waited to die. He succeeded.
Unfortunately children who believe they know all often know very little.
‘I was intrigued by the number of migrants being recruited’?
That’s because our working age permanent population passed the ‘demographic sweet spot’ fifteen years ago, and aged care is not the first choice of occupation for many young or working age Australians.
There is not evidence to suggest that ‘immigration’ is to blame for a less equitable society e.g. Australia has had immigration since 1788, when things were less equitable?
Immigration in. ‘modern’ day Australia is very much tied to inequality. Migrants are used in this industry like many others because they are more easily exploited, labour is an overhead that must be pushed down in order to maximise profit. Unfortunately, one of the many downsides to employing usually poorly trained migrants, who have very little knowledge of bargaining power on the shop floor and/or are easily intimidated by their employer, inevitably leads to very poor outcomes for the customer, that being, the Aged Care customer. Privatisation of this sector has led to the commodification of aged care, albeit, the customer is now a commodity and no longer an individual with specific, intrinsic human needs – do you get it!!! That’s the reality of this ‘NOW’ economic model of Aged Care in Australia. You voted for it and now you’ve got it!! And one day you will be old and more than likely (40-50 per cent likely) will end up in it!! This sector like the NDIA sector should never have been privatised, an equitable user pay system could have been incorporated into these sectors to ensure a much higher level of equity for both the service consumer and those that work within these industries. You can’t change a lemon into an orange, no matter how much you tinker and tweak – it is what it is!! WAKE UP AUSTRALIANS, YOU’VE BEEN FOOLED AGAIN!
The one subject not mentioned at all in these comments is voluntary assisted euthanasia, the right to choose to die with dignity. I wonder how many people, like my parent, just secretly decide to end it all by ceasing to take their medication. There are kinder more dignified ways to die if they were allowed. When the time comes where I can no longer care for myself, and continued living becomes intolerable, I would like to be able to choose to die peacefully, painlessly and with dignity.
Well you can, really. No fluids with a morphine pack is a tried and true defacto VAD without the bullying demaqnds that care staff, medical staff and the wider society be asked to bear some of the moral burden of what is more properly your private business and choice.
Also, that wider society doesn’t send a message to those living with the same condition as you who do NOT agree that their life is not worth living don’t get effectively devalued by that wider human tribe.
By all means elect to die with dignity. You don’t really need VAD to do so.