
Is the Omicron variant a genuine threat with the world just starting to recover from Delta, or has it overhyped fear mongering from vested interests?
The headline is certainly worrying: the mysterious variant has an especially scary 30+ mutations, which some experts fear may make the strain more contagious and potentially able to evade existing vaccines. The urgent threat led to many countries slamming borders shut.
But just how bad is Omicron? Let’s look closely at the reported data.
The variant was first recognised in Botswana on November 11; three days later it was reported in South Africa.
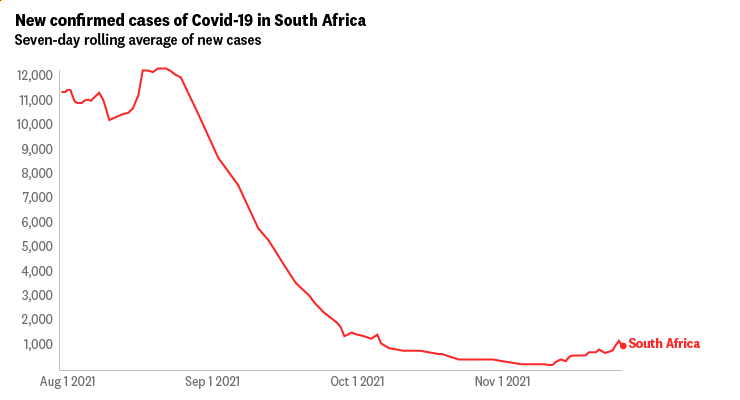
Rolling seven-day infections have increased in South Africa, rising from 262 daily cases to 1691 on November 27 (they have stabilised at 2800 a day since Friday). But there are several problems with this overly simplistic causation-correlation point.
First, looking more broadly, daily COVID-19 infections in South Africa are 92% below August levels:
But when you look at last week’s data, something that really stands out — and you need to look beyond the seven-day smoothed graphs which is what almost everyone uses and consider the reported daily case numbers:
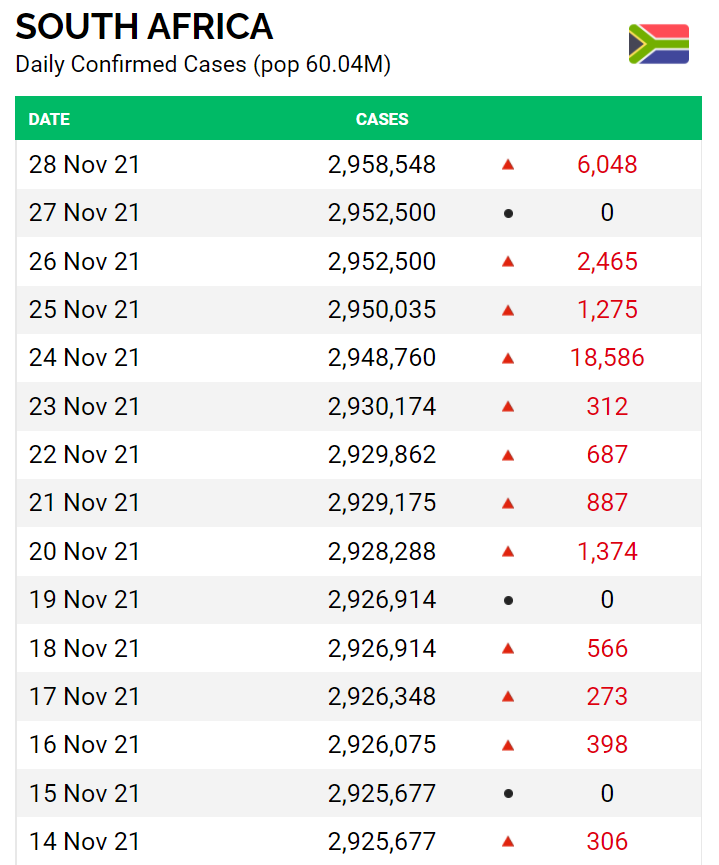
The November 24 figure seems very out of place, and at first glance extremely concerning — until you read this press release from the South African Department of Health on 23 November: “The Department of Health has added the rapid antigen tests on the line of COVID-19 statistics, with effect from today… As we report test data and case numbers for the past 24 hours through our outbreak reporting system, we will observe an increase in a single day, which will create a distortion of the seven-day moving average and an unusual spike on the reporting epidemic curve.”
The South African government foreshadowed an increase in positive cases on November 23 — not just because of Omicron but because it started including positive antigen test results in its daily COVID reports.
On November 23, weeks after the new variant started spreading in South Africa, the positivity rate was a relatively low 2.1%, a fraction of what is being reported in Europe. That rate has certainly increased in the past week, hitting 9.1% on Friday, but it’s difficult to determine how that has been impacted by the increased testing regime. South Africa also has very low vaccine coverage — only 24% of the population are fully vaccinated.
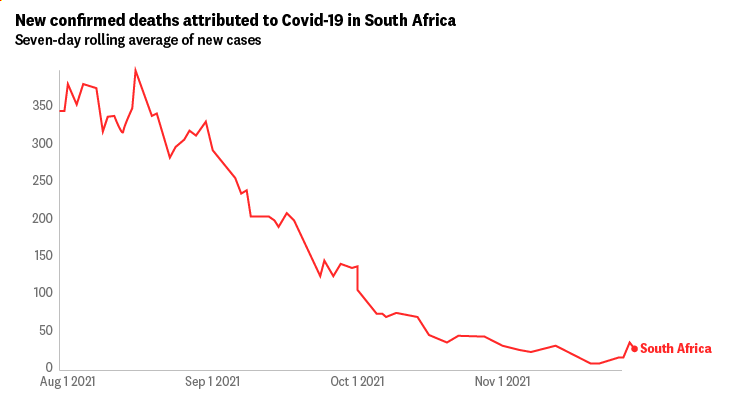
Another way to assess Omicron’s impact is by the movement in fatalities (which, unlike cases, are not affected by changing the testing criteria). Given the average time between infection and death for COVID is 18 days, enough time has elapsed to see some sort of effect on death rates. However, the fatality level in South Africa has dropped since Omicron was first recognised, and remains 92% below the fatality rate in August:
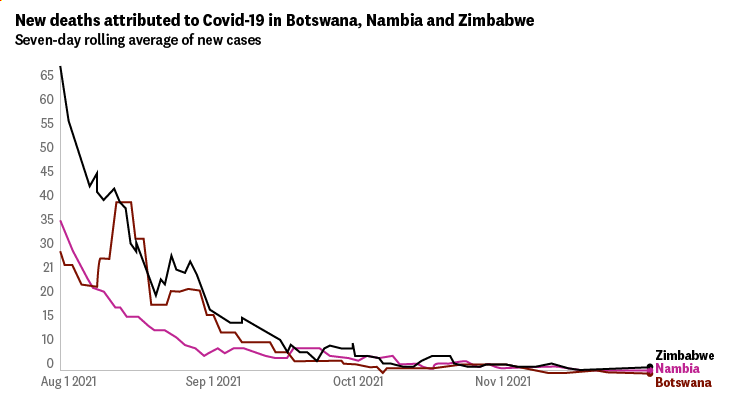
Given the South African data has been affected by the antigen test data, it is also worth considering the other countries that reported the variant. Botswana, for example, reported Omicron three days before South Africa. Here is the rolling seven-day infection levels in Botswana, Zimbabwe, and Namibia:
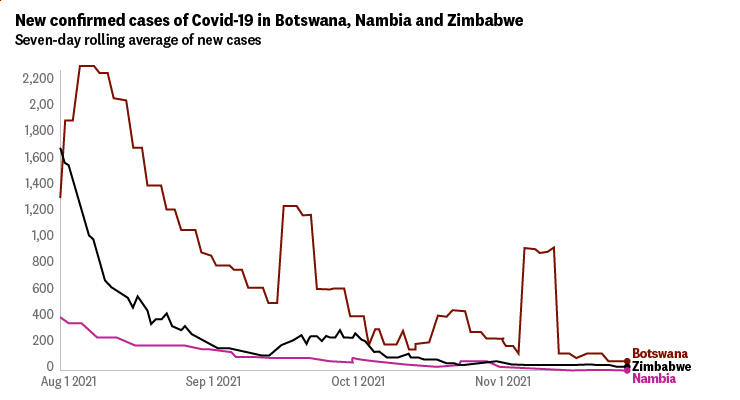
In Botswana, COVID infections have dropped by 97% since August. In Zimbabwe, cases plunged by 98.5%. The fatality count has dropped by even more: Botswana is averaging zero deaths a day. It appears the only thing Omicron has killed in Botswana is COVID itself:
Although it is possible that Omicron is more contagious, and testing data in African countries is less extensive than developed nations (plus the mild nature of the variant may mean there are many undetected positive cases), those concerns do not yet appear to be borne in data from any of the six countries that have been blacklisted by the developed world.
Meanwhile the South African data shows an increase in positive test results occurred only after rapid testing was included.
Dr Angelique Coetzee, chair of the South African Medical Association who first raised the alarm about the new variant, noted that “most of [the patients have] very, very mild symptoms, and none of them, so far, have admitted patients to surgeries. We have been able to treat these patients conservatively at home.”
While the World Health Organization — perhaps still reeling from initial criticism in January 2020 — may have moved too quickly in deeming Omicron a “variant of concern” given the data indicates it appears to cause little or no symptoms and hasn’t spread rapidly through other African nations, there have been some beneficiaries of the action. Within hours of the WHO’s announcement, Pfizer’s share price rose by 10%, adding US$30 billion to its market capitalisation, and Moderna’s share price leapt by 21% in hours, adding US$32 billion to its value.







Umm… Crikey, you know how you’re always chasing the conflict of interest pollies and corporate types? How’s about you stop giving your wealthy board member a voice for his whinging, twisting of statistics and doubting of scientists. He owns a LUXURY TRAVEL COMPANY! This is not journalism, it’s a voice for the business interests of a powerful person in your very own company.
Why let this compromised fool cover this story? Who can take anything he says seriously on this topic? He’s an embarrassment to Crikey and a regular insult to the intelligence and finances of your readership.
Seriously, mate, stick to your day job. Your coverage of Covid issues has been both ignorant and incredibly self serving, and this is amongst the worst of the articles you have written. Of course a new variant is a problem. New variants have always been the fear, and no-one knows how this one might mutate. Your scare mongering about ‘big pharma’ is straight out of the anti vax playbook. There are vested interests in play here. They are totally evident in this article. In all your articles.
This is an excellent article, although not many Crikey commenters will like it. Bravo on Crikey for not toadying to the narrative of their older, risk adverse, mostly retired ex public servant commenter demographic.
Just to complete the circle-jerk: if I hear or read another person spout ‘risk-adverse’ I’ll throw an online dictionary at them.
I don’t like adverse risk. But I am generally risk-averse. Please, learn the difference.
I doubt that Phizer and Moderna had anything to do with it given that the first commentary suggested that their vaccines could be ineffective against the new variant.
That is basic epidemiology – ineffective vaccination is a prime impetus to mutation.
That’s a different type of ineffective vaccination you’re talking about.
I meant outdated, poorly stored, minimal dosages, incomplete courses etc.
In many regions such as Africa cross contamination from reused syringes is common.
But painting Pfizer and Moderna as the compromised villains in the piece is easy – even necessary – when you own a LUXURY TRAVEL COMPANY.
This article looks like it is following the story just long enough to make a point of its own. There’s plenty of info out there right now and this is cherry picking at its finest.